
In Osun State, it’s one doctor per 263,000 patients as the state struggles to deliver medical care.
Despite revitalizing its primary health care facilities, inadequate manpower continues to worsen access to healthcare among Osun State’s teeming population, which is currently put at over five million as revealed by Radio Nigeria correspondent, Adenitan Akinola, in this investigation supported by the Wole Soyinka Centre for Investigative Journalism and the MacArthur Foundation.
Currently, in Osun State, there are over 1,000 Primary Health Centres.
Only 876 of the facilities are functional, out of which 332 were revitalized under the Save One Million Lives (SOML) $20 million Federal Government/World Bank grant obtained by the state government in 2019.
According to an e-document from the Osun State Ministry of Health dated 2021, titled “Data for all CaDr.es in LG” and obtained by Radio Nigeria, there are 19 medical doctors, 17 pharmacists, 19 medical laboratory scientists and 230 nurses; while health assistants are 830 in number and Junior Community Health Extension Workers (JCHEW) are 790, among other categories of workers providing health care services in the 876 functional PHCs across the state with a population of over five million.
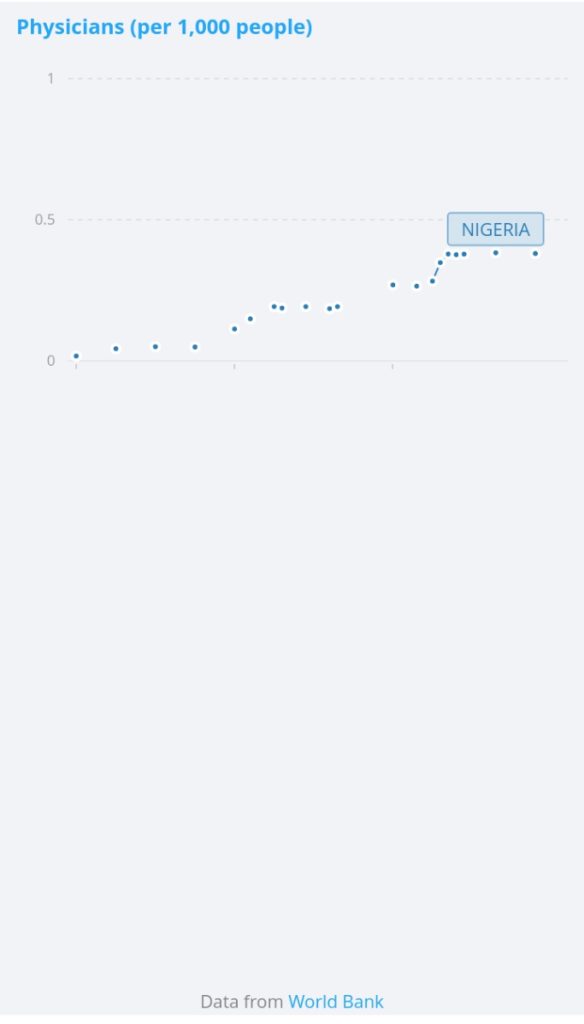
What this translates into is that on average, a medical doctor in Osun State serves no less than 263,000 patients, as opposed to the World Health Organization’s standard of 600 patients to one doctor if patients must enjoy adequate medical attention!
By contrast, the British Medical Association recommends that General Practitioners see a maximum of 15 patients with complex needs per day.
Examples of these include patients with multiple medical problems such as heart failure, diabetes and related kidney disease, frail seniors, and patients with chronic mental health conditions.
In an interview, a community health expert with the Osun State government who identified himself simply as Dr Femi said that most of the PHCs have just between two and three clinical and non-clinical staff, who are majorly Community Health Extension Workers [CHEW] or health assistants.
From Herbal Home to Hospital in Search of Cure
Mrs Omotoso Khadijat, a petty trader single mother had come from Ijana village in Obokun Local Government area of Osun State to Orinkiran Primary Health Center in Ilesa West LG, covering a distance of about 50 kilometres to save her son who had been down for nine days from suspected typhoid fever, having been placed on herbal remedies that had not made the situation better.
She told Radio Nigeria in an interview that she was one of the few lucky ones who could afford such “luxury” of seeking medical care away from the village to save her child.
“I am just lucky that I have little education and I can raise money to come here. Many children are lost to cases like this and our people call it a spiritual attack” . There are no medical personnel in Ijana Primary Health Centre to attend to anyone,” she said, unwittingly corroborating the unwieldy statistics of Nigeria’s child mortality rate, which currently stands at 117 per 1,000 under-five children, according to UNICEF data on www.unicef.org.
Mrs Omotoso noted that residents of Ijana, Ibala and other communities in Obokun LG often come to Ilesa for medical care and those who could not afford transport resort to alternative traditional medical care.
The traditional ruler of the community, the Atarua-elect of Ijana, Oba Olusegun Ogunleye, confirmed the development with a plea to the government to make the only health centre in the community functional.
“There is only one nurse, a female that covers both Ijana and Ibala communities (a distance of about 20 kilometres with a population of over 40,000 people). I will give you her contact to verify my claims”.
The Ijana health centre that was inaugurated with fanfare has been completely abandoned due to the absence of the requisite workforce.

“As a community, there is little we can do to employ healthcare providers,” the ruler stated.
Radio Nigeria put a call across to the number provided by the traditional ruler, but the respondent denied being the person, perhaps for fear of being reprimanded by the government.
The situation is the same at Odeyinka village in Ayedaade local government.
The community, which is about 35 kilometres from Ikire, the local government headquarters, is only accessible by motorcycle.
When Mr Hafeez Kolapo, the motorcyclist that drove this reporter learnt the destination was the health centre, he betrayed his emotions claiming that he lost his pregnant wife early this year when he brought her on an emergency to the newly revitalized health centre where he met only two personnel who he said could not handle the case and there was no means of referral until the pregnant woman died at about nine o’clock in the evening.
“When we got here that night, the whole place was dark. We met a security man and two women who looked like assistants in the place. It was in rage I asked for the doctor on duty, but they said they were the ones on duty. They could not do anything tangible until the women and the security man we met promised to call the nurse on duty,” Kolapo said.
The situation cannot be said to be different in other Primary Health Care facilities visited across some local governments in the state.


Inadequate, Incompetent Manpower
Most of the primary health centres visited were being managed by personnel referred to as Community Health Extension Workers, CHEW, pharmacy technicians and laboratory attendants assisted by N-Power health assistants in some cases.
The CHEW, according to Annals of Family Medicine published by the National Library of Medicine, “are trained individuals with limited to no formal medical education who provide patient-facing support and services in primary care. They carry out functions that are person-centred, support team-based care.”
In the same vein, the N-Power health assistants were workers engaged under the Federal Government N-Power programme to give support to health workers in medical facilities.
At the Alujue PHC in Ede North Local Government, Radio Nigeria met one female CHEW official attending to patients and assisted by N-Power health assistants.
The lady who did not want to be mentioned, but was simply identified as “Aunty Ade’” by the patients, directed our reporter to a notice containing a list of staff.

On the list were eight names comprising of four CHEW personnel, two pharmacy technicians, one laboratory assistant and one N-Power health assistant.
Similarly, at Ara PHC in Egbedore Local Government, an official met this reporter attending to people who simply identified himself as Aderinto, said there were only seven clinical staff members with neither a doctor nor a nurse in the facility that serves a community of about 50,000 people.

“We have only one doctor at the local government that visits once in a while and we call him during emergencies. The seven of us here run two shifts daily, morning and night, with no day off,” Aderinto said.
In some other places, such as Ikonifin PHC in Olaoluwa council, Oteu village PHC in Ifedayo and Safejo PHC in Ife South local governments, there were only between two and three personnel, including the security man, managing the facility.
“Visiting health centre a waste of time” – Community Leader
A community leader in Oteu village, Elder Michael Alabi, told Radio Nigeria that going to the health centre was a waste of time, as one could wait for more than six hours before he could be attended to.
Indeed, most of the health centres visited are headed and managed by the CHEW crew.
Radio Nigeria made efforts to speak with the leadership of the Association of Community Health Workers, Osun State chapter, but the chairman of the Association, Mr Ola Olaniyi, declined comments, saying he can only grant interviews with the approval of the Primary Health Care Board.
However, a Public Health Consultant with the Ekiti State University Teaching Hospital, Professor Olusola Odu, explained that “ordinarily, CHEW personnel should not lead a Primary Health Centre, but in the absence of a doctor or public health nurse, they could be in charge”, adding, “because there is no vacuum in management.”
“There are lower-level facilities like health posts or Basic health centres, especially in rural areas where the only health workers available are CHEWs. In such circumstances, they will be the ones to manage the facility but under the constant supervision of the LGA PHC coordinator who should be a Public Health Doctor,” Professor Odu said.
But from the document issued by the state government, “there are only 17 doctors and 230 nurses in the service of the Primary Health Care Board who are expected to cover the functional 876 PHCs spread across the 30 local governments and one area office of the state.”
“Government making efforts to address the situation” – Osun Health Commissioner
However, the Osun State government did not deny the challenge of inadequate manpower in its primary health centres, but it described it as a national problem, with the assurance that it is making efforts to address it.
The Osun State Commissioner for Health, Dr Rafiu Issamotu, who told this reporter that the government had taken steps to mitigate the consequences of the shortage of manpower at the PHCs, however, noted that the $20 million SOML grant did not cover personnel hire, but it was for basic facility turnaround.
“We can have a situation where the most senior person in a facility is a CHEW. They have been trained to function so that the place will not suffer.”

“We have a policy of Task Shifting/Task Sharing; a situation where a CHEW in our facility can perform the function of a nurse, such as taking delivery of a pregnant woman, even though they are not midwives. They have been so trained.”
“A pharmacist technician should be able to perform the function of a pharmacist, though he knows he is not a pharmacist. In a rural area, they should be able to perform without hitch. This practice is recognised by WHO,” the commissioner stated.
But this practice is at variance with the National Primary Health Care Development Agency Minimum Standard for Primary Health Care in Nigeria, which states that, for a PHC per political ward with a population of 10,000, each PHC must have a medical officer if available, a community health officer, who must work under a standing order, four nurses/midwives, three Community Health Extension Workers who must work under a standing order, one pharmacy technician, six Junior CHEWs who must work under a standing order, one environmental officer, one medical record officer, and one laboratory technician.
This workforce is to be supported by two health assistants, two security and one general maintenance staff.
The Osun State Commissioner for Health, Dr Rafiu Issamotu, argued that the situation at the Osun State PHCs was not that of the dearth of personnel to attend to patients, but that the waiting period could only be long before the few available ones could serve all the patients present.
The commissioner said that two weeks from the period of this interview (Tuesday 7th September), the state government would begin the process of recruiting more clinical staff at the PHCS.
As of the time of filling this story, which is two weeks from the period of the interview, the state government has not commenced employing more staff at the Primary Health Care level.
Adenitan Akinola
Subscribe to our Telegram Channel and join our Whatsapp Update Group


